
In this blog I look into phobias – what they are, where they come from, and how we can treat them.

Tim Kerr, EDIT Lab PhD student
Kerauno, from the Ancient Greek keraunós, meaning lightning.
Phobia, from the Ancient Greek Phóbos, the god of fear and panic.
Linking these two unrelated words together, we get a new concept: Keraunophobia, the fear of lightning.

There is probably no limit to the number of other potential phobias in existence, each with their own characteristic Greek prefixes.
Some are well known; arachnophobia, a fear of spiders, and claustrophobia, a fear of small spaces. Others are known, but probably not by name; glossophobia, a fear of public speaking, or mysophobia, a fear of germs. And some are known probably only to those who experience them. Genuphobia, a fear of knees. Me neither.
Like the words that define them, phobias manifest through the internal association of two usually unrelated concepts. A neutral object or situation gets paired with a negative emotional experience. Then, upon encountering the object or situation again, we re-experience the negative experience, and develop a fear response to it.
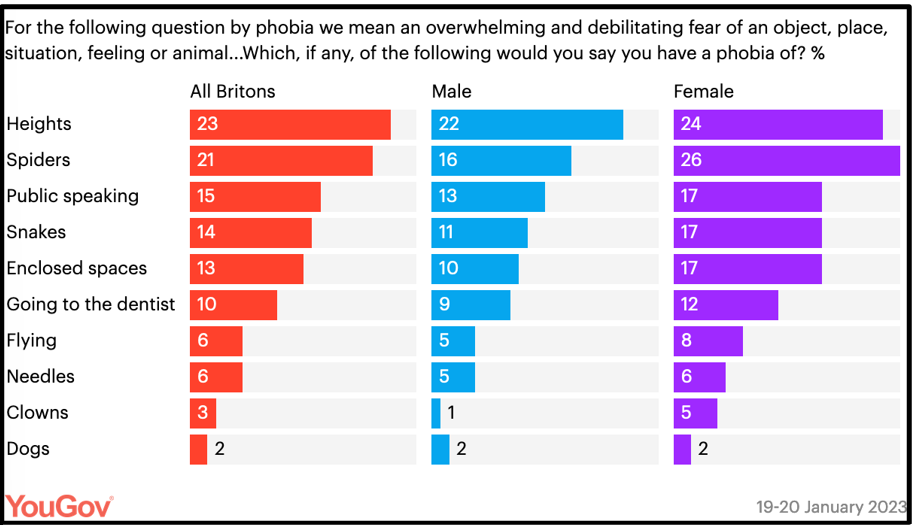
1 – A recent YouGov poll showing some of the more frequent phobias experienced by Britons (1).
Whilst phobias can occur at any point in life, they are predominantly disorders of childhood, reflecting their developmental associations.
There are two prevailing theories on the development of phobias. One proposes that phobias are learned, or to use the psychological term, conditioned. This states that the object or situation is experienced alongside an unpleasant or dangerous situation, and a phobic association is made. A child bitten by a spider in a particular room, might then be conditioned to be wary of that room in the future.
This theory cannot explain all phobias. Notably phobias of the natural environment, such as the fear of lightning or of heights, tend not to result from directly experiencing pain or trauma alongside the object.
Another prominent explanation of the development of those phobias, is modelling. Here, phobias develop through witnessing others react fearfully to objects or situations. A parent showing fear towards a spider might be observed by their child, who then begins to display a similar phobia towards spiders.
Interestingly, fears of natural phenomena, such as a fear of animals or weather, tend to occur at younger ages, whereas more abstract fears of height or flying have a later age of onset. This might suggest both theories hold some validity, and that the process may differ for specific types of phobia.

2 – Arachnophobia, as depicted by the AI image generator DALL-E. Though, I only count 4.5 legs on this spider, which is perhaps more unsettling.
Twin studies are well suited to examine whether phobias follow the learned (non-shared environment) or modelled (shared environment) pattern of development. Alas, as is often the case, there are too few studies looking into these phenomena, amplified by the specific, individualised nature of phobias, to draw any firm conclusions.
One review suggests that the shared environment accounts for the expression of childhood phobias, pointing to modelling (2). It also suggests genetic factors better explain adulthood phobias, pointing to conditioning. This is backed up by meta-analysis, which interestingly demonstrates differing heritability estimates dependent on the type of phobia (3).
For instance, the highest heritability estimates seem to occur for blood, injection, or injury phobias, with genetic and non-shared environment explaining far more of the variance than shared environment.
In a small percentage of those with phobias, the fear response becomes pathological, and significantly interferes with normal life. This might lead to a diagnosis of specific phobia.
Specific phobias typically involve excessive anxiety or fear in anticipation of, or following, exposure to specific objects or situations accompanied by avoidance of that object or situation. There will typically be an associated somatic fear response, including heart rate elevation, sweating, and goosepimples.

3 – Some can overcome their fears, and achieve great things. As an aside, this picture always gives me goosebumps, a mild version of the somatic fear response I describe in text. Photograph by Jimmy Chin (4)
The first line treatment for specific phobia aims to reverse the associative learning process. Exposure therapy, a component of cognitive behavioural therapy (CBT), is a graduated process of showing the phobic person a mild form of the object. If the mild fear response this generates is tolerated, the participant is later shown increasingly extreme versions of the object. This approach is shown to be more effective than treatments involving imagining the object, or virtual reality approaches.
Through our ongoing work using the FLARe app, we aim to look deeper into the associative learning mechanisms underlying fear conditioning. This may shed light on why phobias develop in some and not others, and could even point to where treatment might be most effective.
References:
(1) https://yougov.co.uk/topics/society/articles-reports/2023/02/27/what-do-britons-say-they-have-phobia
(2) Eaton, W. W., Bienvenu, O. J., & Miloyan, B. (2018). Specific phobias. The Lancet Psychiatry, 5(8), 678–686. https://doi.org/10.1016/S2215-0366(18)30169-X
(3) Van Houtem, C. M. H. H., Laine, M. L., Boomsma, D. I., Ligthart, L., van Wijk, A. J., & De Jongh, A. (2013). A review and meta-analysis of the heritability of specific phobia subtypes and corresponding fears. Journal of Anxiety Disorders, 27(4), 379–388. https://doi.org/10.1016/j.janxdis.2013.04.007
(4) https://nautil.us/the-strange-brain-of-the-worlds-greatest-solo-climber-236051/