
Researchers from EDIT lab and the Twins Early Development Study have just published an article about the genetics of the ‘p factor’ across childhood and adolescence. What is the p factor and what did they find?
The p factor
Individuals who score highly for certain psychopathological traits tend to also score highly on others. Individuals diagnosed with one psychiatric disorder are more likely to be diagnosed with another within a year’s time, and therapies and medications are often not diagnosis-specific (e.g. selective serotonin reuptake inhibitors for depression, anxiety and eating disorders). Many researchers think that these overlaps may be explained by a single latent factor that reflects general liability to a wide range of psychopathologies: the p factor. This is not a new idea (it goes back to the 20th Century) but has recently become a popular research area for developmental psychologists and behavioural geneticists. Indeed, twin and family studies suggest that covariation between forms of childhood psychopathology can be substantially accounted for by genetic risk factors common across disorders.
However, little is known about the genetic and environmental architecture of general psychopathology across childhood and adolescence, and the extent to which a general p factor in earlier development relates genetically to adult psychiatric disorders. The Twins Early Development Study (TEDS) provided a perfect opportunity to take a systematic look at the structure of the p factor across development, due to the richness of the data. TEDS has collected diverse measures of behaviour problems (depressive traits, emotional problems, peer problems, autism traits, hyperactivity, antisocial behaviour, conduct problems and psychopathic tendencies), rated by children, parents and teachers at ages 7, 9, 12 and 16.
We had three key questions and answers.
- How does p manifest across diverse measures, raters, ages?
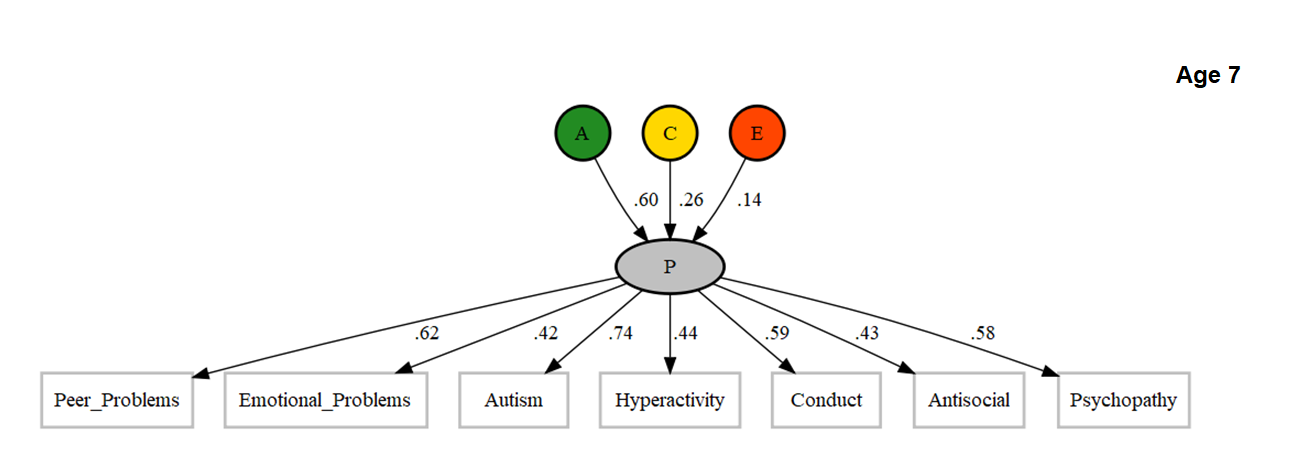
Using common pathway twin models, we found that a substantially genetically-influenced general psychopathology factor could be identified across different measures, raters and ages. For example, the figure below shows that parent-reported measures of child psychopathology at age 7 all loaded on a common p factor (loadings >0.4), which was strongly heritable (60%). Overall, p manifests consistently, although there is still some specificity, indicated by residual variation not accounted for by the p factor.
- How much do genes and environments contribute to stability in p across ages?
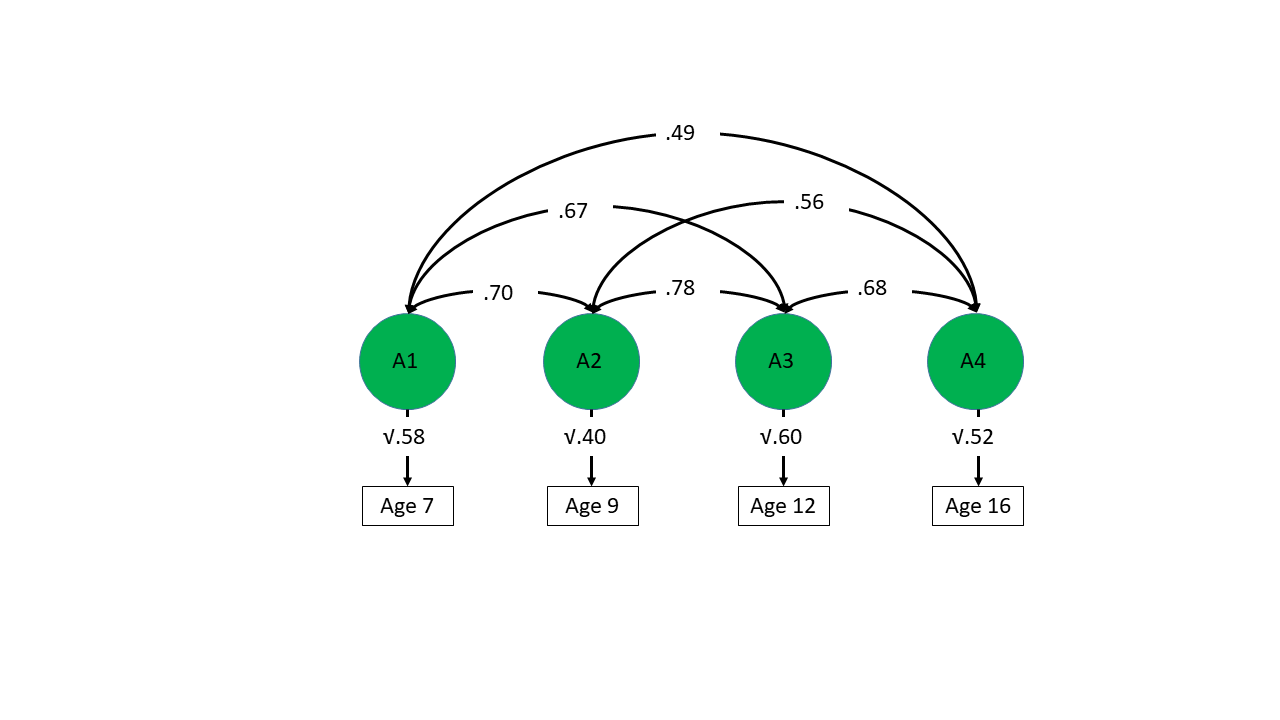
Using another type of multivariate twin model – the longitudinal Cholesky decomposition – we found that there was a common genetic component linking measures of p at ages 7, 9, 12 and 16. The figure below shows that p at each age was genetically correlated with p at other ages. This indicates that genetic factors explaining individual differences at one age also explain individual differences at the other ages, although again there are age-specific genetic effects left over, as the genetic correlations are not 1. The difficulty with this analysis was that slightly different measures were available at each age, and also that measures mean different things at different ages (this is known as measurement invariance). However, exactly for this reason, we think that these high genetic correlations are even more striking.
- Do polygenic scores, based on risk for typically adult psychiatric disorders, predict p in childhood?
We wanted to extend the insights from twin model fitting across TEDS ages 7-16, to see whether the genes influencing the p factor in childhood and adolescence are also linked to general genetic risk for psychiatric disorders in later life. To do this, we generated measures of participants’ genetic risk for typically adult psychiatric disorders – polygenic scores. We then took the first principal component of these polygenic scores to index what is common across them (see figure below), and tested its associations with phenotypic p factors in childhood and adolescence.
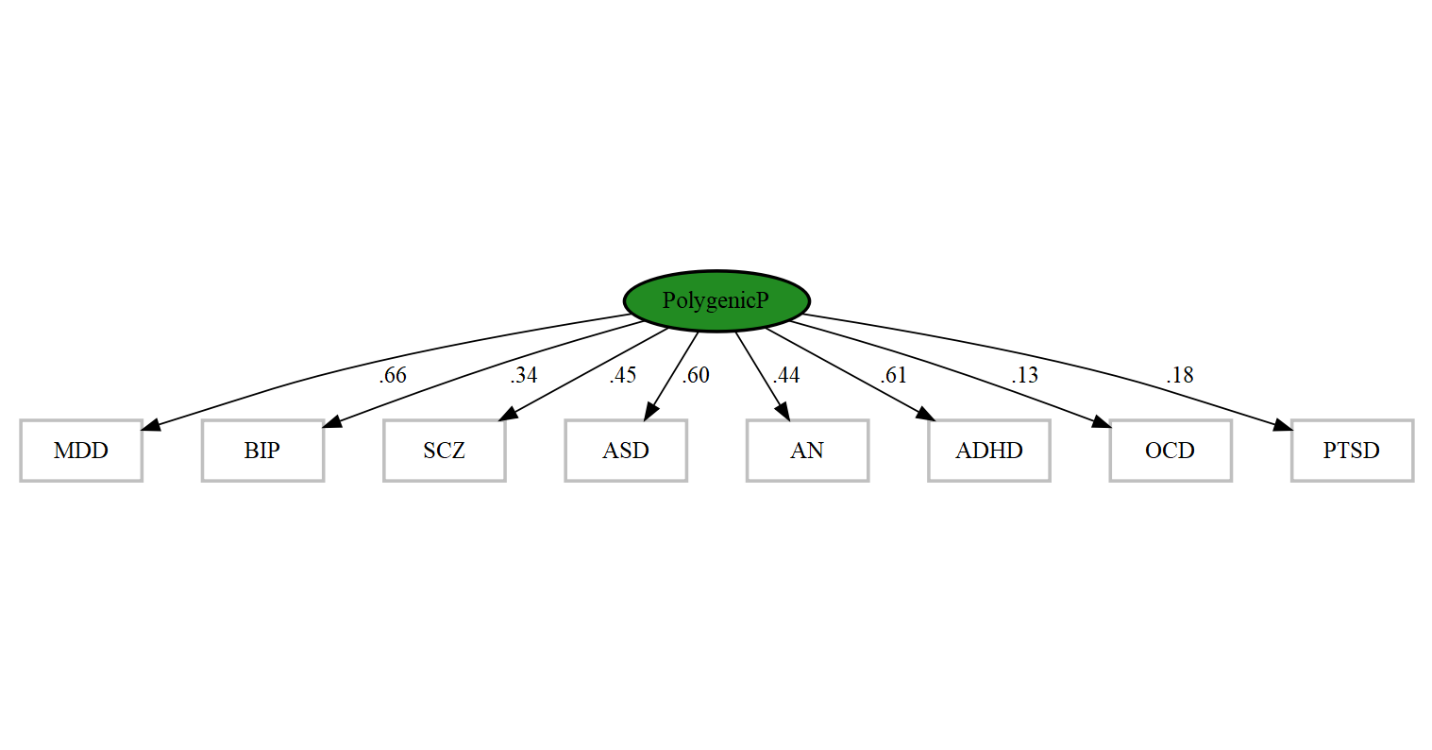
NB: labels stand for: major depression, bipolar, schizophrenia, autism, anorexia, ADHD, obsessive-compulsive disorder, and posttraumatic stress disorder polygenic scores.
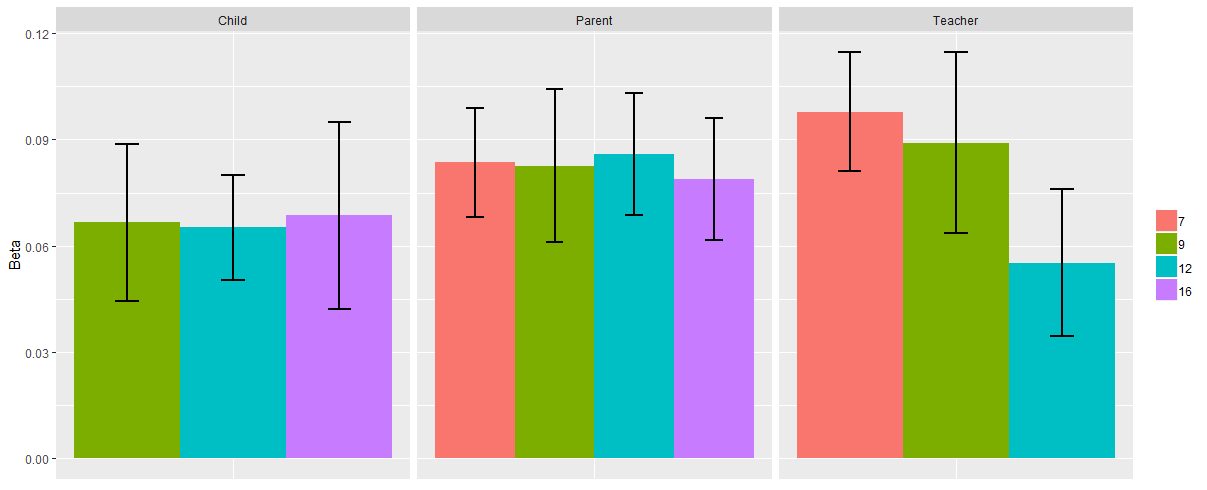
The figure below shows that there are shared genetic influences connecting general risk for (mostly) adult psychiatric disorders that are unmeasured in our sample, and childhood psychopathology (each bar represents phenotypic p for each age/rater in TEDS). These associations are consistent across ages in childhood and adolescence, and across raters. The variance explained by ‘polygenic p’ is low (~1%), but is within the expected range considering previous research in this area.
This suggests that genetic risk for psychiatric disorders emerges in childhood, in the form of continuously measured behaviour problems.
The idea that a common genetic liability for psychopathology has genetic influences across the lifespan has implications for research and clinical practice. For example, the p factor (polygenic or phenotypic) might be used as control variable in research studies aiming at isolating risk factors for specific diseases. In practice, identification of individuals at risk may be easier by assessing general psychopathology dimensions. Clinicians might want to assess symptoms from a variety of disorders, not only the one diagnosed (see also https://onlinelibrary.wiley.com/doi/abs/10.1111/jcpp.13063).