
Fear is an emotional response vital for our survival. However, overwhelming fear can lead to excessive avoidance of situations that are not actually dangerous, causing distress and impairing daily functioning. Here, we give an overview of fear, explaining when it becomes pathological and how it can be studied experimentally.



Fear
Fear is a powerful emotional response to real or perceived imminent threat or danger. Fear triggers multiple reactions in our body, working through the rapid firing of nerves (via the sympathetic nervous system) and through the release of ‘stress hormones’ (adrenaline and noradrenaline – the adrenal-cortical system). Together these pathways get our hearts racing, our muscles tensing and generally prime our body to respond to the threat in the most efficient way possible (you’ve probably heard of the fight or flight response). The behavioural response varies depending on the organism and the situation. For example, we may defend ourselves (fight), escape to safety (flight), or even freeze (some scientists think this could give us time to consider options, or might kick in when neither fighting nor fleeing are possible).

Although fear is about responding to danger, it definitely isn’t all bad. Being able to experience fear has saved individuals of our species (and others) more than once through our evolutionary history; and Hollywood and amusement parks have cashed in on the pure enjoyment some people experience in the face of (controlled) fear. While fear can be vital for our survival, helping us adjust to the environment, it can also become pathological when the experienced fear is disproportionate to the actual threat or danger and disrupts an individual’s functioning (this is the definition in the official diagnostic manual – the DSM-5).
Fear vs. Anxiety
Overwhelming fear can feel a lot like intense anxiety. This is because both experiences are closely linked and even overlap. As mentioned above, fear causes the activation of a defense response system in the face of imminent danger or threat. On the other hand, anxiety can be thought of as a response to the anticipation of a potential, future threat. Anxiety disorders share features of both pathological fear and anxiety, and are mostly differentiated by the content and situations evoking the emotional response (DSM-5). This content can range from specific objects or environments, i.e. specific phobias (heights, small enclosed spaces, spiders and other creepy crawlies, to name a few), to social situations (social anxiety), or even general worries about events or activities (generalized anxiety). Recent initiatives to identify the physiological profile of anxiety disorders show that these disorders can be seen on a spectrum with more focal, specific fears on one end (specific phobias) and more diffuse, general distress on the other (generalized anxiety; McTeague & Lang, 2012). Thus, fear and anxiety can have different implications in prognosis and treatment of anxiety disorders.
Experimental research on Fear: Fear Conditioning
Pathological fear as seen in anxiety disorders is thought to emerge when fear responses to danger are inappropriately associated with stimuli or situations that are actually harmless for the individual within a specific environment (Ohman & Mineka, 2001). Therefore, the learning of associations among stimuli or situations is a core mechanism underlying the development of pathological fear and anxiety. The most fundamental process of associative learning that has been examined in relation to anxiety and fear is classical conditioning. This goes back to the research of Russian physiologist Ivan Pavlov in the early 1900s. While studying digestive processes in dogs, Pavlov noticed that the dogs began salivating whenever they saw the person that usually fed them. This showed that the dogs had made an association between the person and the food. This was the beginning of a series of experiments on what was later termed classical conditioning, i.e. the pairing of a neutral stimulus (e.g. the sound of a bell) with a biologically significant stimulus that elicits an automatic response (e.g. food eliciting salivation).
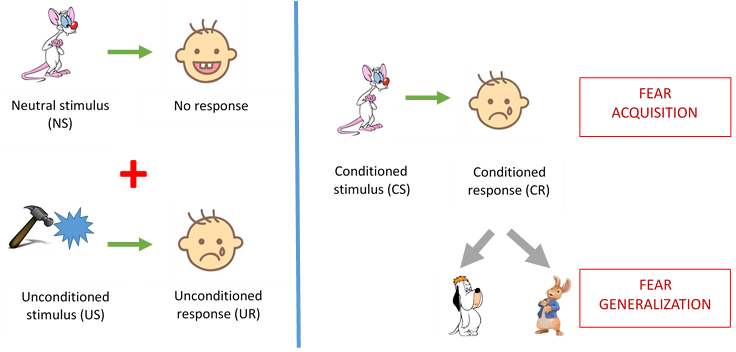
The principles of classical conditioning were soon used to study associative learning in the context of fear. John Watson, for example, used Pavlovian conditioning to induce fear towards furry animals in a toddler called little Albert in the 1920s (see figure below). Specifically, he repeatedly presented a white lab rat to little Albert along with a loud banging noise, which automatically elicited a fearful response by the toddler. After multiple presentations, little Albert learned the association between the rat and the noise, so he started showing fear even in the presence of the rat alone. What’s more, little Albert was now afraid not only of the lab rat, but also of other furry animals like rabbits or dogs. This generalization of fear to other similar stimuli, is considered to be a mechanism by which pathological fear perpetuates.
Researchers have since extended this basic paradigm to study (under controlled experimental conditions) how people acquire fears in real life and how these can shape into psychopathology. A meta-analysis of studies examining these processes in patients with anxiety disorders has shown that patients with anxiety tend to generalize the fear they acquired towards a specific stimulus which was paired with something aversive (called a CS+ in fear conditioning nomenclature), to another stimulus that was never paired with anything unpleasant (called a CS-; Duits et al., 2015). While healthy individuals learn that the second stimulus is safe, patients with anxiety cannot restrict their fear responses (Duits et al., 2015).
Fear conditioning and treating anxiety
One of the most common ways to treat anxiety, especially phobias, is through exposure therapy. Exposure therapy is a form of behavioural intervention whereby the patient suffering from a particular phobia is repeatedly exposed to the feared situation (or stimulus) with the support of a clinician. This exposure is gradual and takes place over numerous sessions. For example, a patient suffering from a phobia of using the elevator might begin by taking trips with the clinician to simply push the button calling the lift, after a few attempts they might try standing in the lift on the ground floor, followed by taking the elevator up one floor, and so on. This repeated, gradual exposure eventually helps the patient to associate their perceived threat with a new meaning, that of safety. Essentially, exposure therapy helps the patient begin to change their expectancy of harm to the feared situation or stimulus (Hofmann, 2008).
Within the fear conditioning experimental paradigm we can model exposure therapy during a phase known as ‘fear extinction’. Fear extinction can take place after a stimulus has been conditioned to elicit a fear response (i.e. once a CS+ has been produced). During extinction, the CS+ is repeatedly presented in the absence of any aversive stimulus so that it no longer predicts danger or discomfort. Gradually, over time, the participant will begin to learn this new pattern and their expectancy of harm will reduce, modelling the process of exposure therapy. In the meta-analysis mentioned earlier (Duits et al., 2015), it was shown that patients with anxiety disorders took longer than healthy individuals to reduce their expectancy of harm to the CS+ during extinction. This delayed ability to extinguish the connection between the CS+ and the aversive stimulus in anxiety disorder patients may explain why, in some cases, their fears can persist for so long despite repeatedly demonstrating they do not pose any harm.
The origins of individual differences in fear and fear conditioning
Twin studies have allowed researchers to estimate the relative influences of genes and environment on the development of phobias and fears. The twin design allows us to estimate heritability (which will be explained in our “H for Heritability post” in two weeks!). Twin studies of specific phobias and their related fears find an average heritability of between 25% and 45% (although individual studies find heritability estimates as low as 0% and as high as 71%). One small twin study has been carried out on fear conditioning so far finding a heritability of between 35-45%. More work is being done (in our group and others) to try and establish the heritability of fear and fear conditioning processes using twin and even SNP heritability approaches – so watch this space!
Conclusion
Although fear itself is a universal and adaptive response to the world around us, pathological fear as seen in specific phobias and anxiety disorders can be quite disabling. For a quick overview of phobias check the NHS website. Specific phobias can be treated using exposure therapy with fairly high efficacy. Experimental research using fear conditioning procedures has been instrumental in this success, but still more research is needed to explore more complicated fears, to understand the aetiology of pathological fear and to maximize treatment efficacy.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). American Psychiatric Pub.
Duits, P., Cath, D. C., Lissek, S., Hox, J. J., Hamm, A. O., Engelhard, I. M., … & Baas, J. M. (2015). Updated meta‐analysis of classical fear conditioning in the anxiety disorders. Depression and anxiety, 32(4), 239-253.
Hofmann, S. G. (2008). Cognitive processes during fear acquisition and extinction in animals and humans: Implications for exposure therapy of anxiety disorders. Clinical psychology review, 28(2), 199-210.
Mignon-Grasteau, S., Chantry-Darmon, C., Boscher, MY. et al. Behav Genet (2017) 47: 114.
Öhman, A., & Mineka, S. (2001). Fears, phobias, and preparedness: toward an evolved module of fear and fear learning. Psychological review, 108(3), 483.